

Hint: It’s a lot more significant than we get credit for.
The most recent CDC data (2015) regarding the C-Section rate puts it at 32.0% of all births in the U.S.. This is more than three times World Health Organization recommendations. The American College of Obstetricians and Gynecologists have done some very commendable work in releasing important practice recommendations for reducing the Cesarean rate (1) and (2). But what is the L&D Nurse’s Role?
NURSES HAVE AN IMPACT.
Nurses are the most common denominator when it comes to childbirth in the United States. 99% of births are attended by L&D nurses. While there is very little research about our role, we are far from neutral bystanders. We are active participants in the process of labor and birth in the U.S., and our work has an impact on every measureable quality indicator.
PAY ATTENTION TO THE NURSES.
Before I describe solutions that are unique to the nurse’s role, I would first like to describe obstacles in the way of these solutions.
#1: LACK OF EMPHASIS ON THE SIGNIFANCE OF THE BEDSIDE NURSE’S ROLE.
What nurses do at the bedside is important. Yet our role can be diminished by the misbelief that since we aren’t creating the plan of care (the set of orders the MD or midwife writes for the care of the patient) that we don’t affect the plan of care. In my ten years of practice as an L&D nurse, I’ve discovered this couldn’t be further from the truth.
#2: “BRAIN DRAIN” OF THE BEDSIDE RN’S EXPERTISE
Obstacle #1 directly impacts obstacle #2. Since the importance of the bedside nurse is diminished, RNs that are passionate about improving birth outcomes are actively encouraged to pursue new roles, such as leadership roles or further education in advanced-practice nursing (like nurse-midwifery).
This shift away from the bedside is problematic for two reasons. First, while the midwifery model of care (especially prenatally) shows superior outcomes, only a small percentage of births are attended by CNMs in the U.S.. Second, when RNs move into leadership, or supervisory roles, they often get mired down with the institutional obligations of that role, rather than being able to actively work to improve birth outcomes on the bedside nursing level. Nurses in supervisory roles are overwhelmed by the mere functioning, planning, staff and budgetary constraints involved in managing a unit; stressors which are only increasing as healthcare system resources become more constrained.
#3: DEFENSIVE NURSING PRACTICE
Defensive nursing practice, or nursing practice that prioritizes the minimization of legal risk above all else, seriously constrains a nurse’s ability to practice the kind of attentive care that women desire — and need — while giving birth. Research shows that continuous support has a dramatic effect on birth outcomes … reducing the Cesarean rate, reducing need for pain medication, and even improving neonatal apgar scores. Yet defensive nursing practice — which is accomplished through tedious, repetitive and nearly all-consuming nursing documentation — constantly draws a nurse’s attention away from his/her patient’s needs, thereby depriving them of the precious presence that women require to safely give birth.

Photo: Paul Golangco – http://www.paulgoimages.com
UGH. ARE YOU FRUSTRATED YET? ME TOO.
Luckily it’s not all bad news.
I’m not a researcher, professor, or public health specialist. I’m #justanurse. But I’ve helped thousands of women give birth the past 10 years, and I pride myself on what I consider to be a unique skill-set I’ve developed over that time to help the most “stubborn” babies be born vaginally.
WAYS THAT BEDSIDE NURSES CAN FACILITATE PHYSIOLOGIC BIRTH
#1: RETHINK THE 3 P’s
In our training as obstetrical nurses, we learn that labor progress is affected by 3 factors: 1) the Passenger – the baby, specifically the baby’s head circumference, position in relationship to mother’s pelvis, and ability to mold; 2) the Pelvis – the mother’s pelvis and it’s shape and internal diameters, and 3) the Power of the contractions.
When it comes to the pelvis, we learn that are specifically 4 kinds, as if God is a manufacturer and there are only 4 models available. We learn that the gynecoid pelvis is ideal for child-bearing, while the android pelvis makes vaginal birth close to impossible.
When it comes to the power of contractions, we imagine the uterus as like a machine, that has a finite amount of power on its own. If spontaneous contractions aren’t powerful enough, then Pitocin is administered. Nurses are all-too familiar with the exhausting refrain of “What’s the Pitocin at?” As if the amount of Pitocin titrated has a direct and uninterrupted effect on the progress of the labor (if only that were true).
LET ME SUGGEST THAT THERE ARE MORE P’S AT PLAY.
#1 – THE PSYCHOLOGY & PHYSIOLOGY OF LABOR (also known as the mind-body connection)
Women’s bodies are very wise. If women don’t feel safe in early labor, (or active labor for that matter), their stress hormone levels rise. Stress hormones (adrenaline, cortisol) have the opposite effect on the body that labor hormones (oxytocin) do — stress hormones will shut down the labor process, telling a woman when the environment is not a safe place to give birth.
Factors that increase maternal stress hormone levels in the birth room:
- Opening and closing the door without announcement.
- Strangers walking into the room, assuming their presence is welcome (can include medical students, nursing students or a rotating array of OB residents.)
- Bright lights in the room.
- Alarms going off without being silenced.
- An audience. Birth is not a spectator sport. Women need privacy to give birth.
- Whenever I arrive in the birth room, I do a “vibes” scan. How many folks are in there? How supportive are these people? How helpful, tuned-in are these people to the woman’s needs? How oblivious are they to her needs (eating strong-smelling foods like French fries and cheeseburgers, yelling at each other, having loud conversations, watching violent television shows.)
- Invasive procedures (think vaginal exams, speculum exams, IV start, lab draws, artificial rupture of membranes) — especially when the woman has not been offered informed consent.
- Note: vaginal exams can be much more traumatic for some women than for others. For women with a history of sexual assault or violence, a vaginal exam can trigger memories of the assault. (Note: far more women have this history than disclose it.)
A NOTE ON INFORMED CONSENT & BIRTH PLANS
As nurses it is beyond our scope of practice to offer informed consent. This doesn’t mean we can’t facilitate informed consent. PATIENT EDUCATION is an essential part of our role. We can “stop the line” before a procedure is performed to ensure that the patient verbalizes understanding of what’s about to happen, and has the opportunity to ask any questions she might have about the procedure. Unless it is a medical emergency (the fetal heart rate is bradycardic and not coming back up, the woman is actively hemorrhaging), it is our legal duty as healthcare professionals to ensure the patient understands what’s going on, and to make sure she consents before the procedure starts.
As much as we healthcare professionals “roll our eyes” at the concept of a birth plan, it’s important to remember that a birth plan is a legal document. For example, if a woman puts in writing that she does not want an episiotomy performed and a provider performs one anyway without her verbal consent, this could be considered assault in a court of law.
#2: POSITIONING TO FACILITATE LABOR PROGRESS & FETAL DESCENT.
When I refer to “positioning,” I’m not just referring to the baby’s position in the mother’s pelvis. I’m also referring to the mother’s position in relationship to gravity.
We do have wonderful research about the benefits of active movement during labor, which Lamaze International emphasizes as one of their Healthy Birth Practices. Unfortunately there is a disconnect between this research finding and actual, bedside nursing practice.
POSITIONING WITHOUT/BEFORE AN EPIDURAL
Unless a patient actively advocates for her ability to move freely (i.e. “has a birth plan”), nursing habit will be to tether her to unnecessary equipment: an IV solution dripping regardless of the mother’s hydration status, continuous fetal monitoring despite a reactive NST, blood pressure cuff in place and going off every 30 minutes without any medical indication to do so. Each of these interventions unnecessarily restricts a woman’s movement.
Nurses are trained and audited on their assessment of patient’s pain scores, and educated to document an intervention whenever a patient states their pain is greater than their acceptable pain score. On a busy unit, the easiest intervention is to first offer an oral or IV pain medication, and if that doesn’t work, to offer an epidural. However, often a patient’s pain can be alleviated by non-pharmacologic interventions (especially in early labor) such as movement — dancing, swaying, walking, sitting on a birth (medicine) ball; repositioning with a peanut ball or pillows; or use of water for pain relief — hopping into the bath or shower. I’ve personally found that this is often all that’s needed!
Especially if a patient is in early labor and may be ruled-out and discharged home, it is essential for a nurse to teach basic comfort measures, to alleviate anxiety about coping through contractions at home, and to empower a woman and her partner to “tune in” to the woman’s body so that she can allow labor to unfold without unnecessary intervention.
During “rule-out labor” discharge teaching I also outline the benefits of staying home in early labor as long as possible: that a woman will be more comfortable in her own environment. I frame my teaching with the goal of returning the power to her, since she was the person who was capable of nurturing the pregnancy, she can now practice trusting her body, that her labor will unfold as it should.
POSITIONING WITH AN EPIDURAL
Many nurses are under the impression that once a woman is comfortable with an epidural, that she is “all tucked in” and doesn’t need as much attention from the nurse. I do advocate for my patients to rest during labor whenever possible. Especially in the middle of the night, I try to “cluster care” so that I’m not constantly opening and closing the door and disturbing that rest. However, patients with epidural anesthesia need to be ACTIVELY managed, just as they would without an epidural.
PATIENTS WITH AN EPIDURAL NEED TO BE FREQUENTLY REPOSITIONED, AND UNLESS THEY ARE 1-HOUR OR LESS POST EPIDURAL (or 1/2 hour post-epidural redose), THEY SHOULD NEVER BE ON THEIR BACK, OR EVEN IN A LEFT OR RIGHT TILT POSITION.
Enter the Peanut Ball.
A 2015 study found that woman who were positioned during labor with a peanut ball had a significantly shorter first stage labor time compared to the control group. Second stage of labor was also significantly shorter. 21% of women assigned to the control group had Cesarean surgery compared to 10% of the women positioned with the peanut ball.
(Note this study was relatively small. But I have seen the same results in my own nursing practice.)
A NOTE ON OCCIPUT POSTERIOR-POSITIONED BABIES AS A CAUSE OF “FAILURE TO PROGRESS”
I cannot even count the number of times I’ve heard the following words come out of a physician’s mouth: “She is persistent OP. I don’t think she’s going to make it [give birth vaginally].”
Out of curiosity, I always pay attention to the baby’s position at birth when a Cesarean is performed for “arrest of descent.” 95 times out of 100 (my estimate), the baby emerges in ROP position.
A Clinical Scenario
I, unlike my peers, am unperturbed by a baby that enters a mother’s pelvis at the start of labor in ROP position. Many babies do. Often-times, I’ve witnessed that these babies will present with ruptured membranes, a high station (-3, at least), and minimal dilation (1-2cm) at the start of labor. Without positional intervention, these babies will also “arrest” around 6-7-8 cm dilation, at -2, -1 or 0 station. Typically this happens after many long hours of labor, back labor that requires epidural anesthesia (with multiple redoses) for pain relief, and membranes ruptured far longer than most of us are comfortable with. For many years of my nursing practice, I would watch as everyone on the care team threw up their hands in this scenario, and became resigned to the fact that the woman would need a C-Section.
Gail Tully, of Spinning Babies and Sharon Muza, of the Miles Circuit, truly changed my nursing practice, allowing me reframe how I think, and intervene, in this situation. By utilizing their positioning techniques in labor, I came to witness first-hand how babies that present in ROP move through their mother’s pelvis in a very predictable way, and help guide them through those movements through strategic positioning.
The Fetal Rose, by Gail Tully ~ http://www.spinningbabies.com
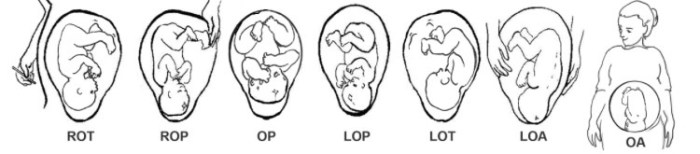
The secret to helping babies in persistent OP position be born vaginally — 1) it takes a really long time, and 2) they have to rotate through the pelvis in a specific direction (clock-wise, from the mother’s perspective). (See the illustration above.)
OP RULES
- Babies in labor have to move from ROT, to ROP, to OP, to LOP, to LOT, to LOA, to OA. It is much, much more uncommon for a baby to go from ROT to ROA than it is for it to have to “take a trip around the world.” This has to do with the mother’s anatomy including her bony pelvis, inlet diameters, the position of pelvic organs (including the sigmoid colon and bladder) and the fact that sometimes, the whole diameter of the baby’s head has to mold before he can fit through the smallest dimensions of the mother’s pelvis (kind of like how a pencil has to rotate to get sharpened.)
- The mother will feel rectal pressure (with or without an epidural) long before its time to push. Contrary to popular belief, rectal pressure before full dilation is a sign of progress in an OP labor … the baby has to move through direct OP (where the occiput will put pressure on the pudendal nerves and cause an urge to bear down / need to poop).
- This rectal urge will not go away until the baby rotates from OP to LOP to LOT. When mom feels this rectal urge, she should avoid squatting, toilet sitting, or any other position where the urge is made stronger. (If she “goes” with the rectal urge, she may swell her cervix and wedge the head further down, so that it’s much harder to rotate out of direct OP.)
- In direct OP position, a mother should be assisted into a forward-leaning inversion (without an epidural) or to a left-side lying position with a large-diameter peanut ball. An alternative if you don’t have a big peanut ball available is to assist the woman to lay on her left side with her right calf cradled in one of the hospital stirrups. The right leg should be on the peanut ball or stirrup in a lunge-like position (up to the sky as we say) with her left leg straight and the woman turned so that she is nearly laying on her stomach.
It sometimes takes 1-2 hours for a baby to rotate from ROP to LOP. Through some practice I’ve learned that it is more effective with an epidural to have the mother maintain the left side-lying position for up to 2 hours without changing it. Contractions should be strong enough at this time (thanks Pitocin) to help rotate the head.
5. Once the baby has rotated from ROP or LOT, life is a walk in the park! I use Leopold’s and as needed, cervical exam to assess for this change. Usually after this rotation, the baby will move from 0 to +1/+2 very quickly. I’ve found that once we’re able to do this, especially if we then “labor down” on her right side with the peanut ball (allowing the baby’s head to rotate from LOT to LOA to OA), the mother typically only has 30 minutes of pushing to do.

Photo courtesy North Dallas Doulas ~ http://www.northdallasdoulas.com
#3: PRESENCE
Sometimes a patient will be grimacing with pain, and what she really requires is simply a reassuring presence. I cannot overemphasize the impact of a the nurse sitting with a woman through several contractions, teaching her how to relax different parts of her body, teaching her the benefits of active movement during early labor, and teaching her partner how to apply counter-pressure or massage.
We nurses are capable of so much, yet, a huge amount of education that I offer my colleagues is awareness of the limits of our role. Regardless of how passionate we nurses are about birth and supporting our patients, the physical-emotional-mental demands of our job description on the average day make it impossible to provide the kind of support women need.
That’s why I’m such a huge advocate for DOULA support, and collaborating with doulas to improve birth outcomes.
Both ACOG and Lamaze International are pro-doula, it’s time for us nurses to be pro-doula as well. A huge obstacle to this are misconceptions on BOTH the nurse’s and the doula’s part about what the other should be doing, and what they shouldn’t. It is an ongoing process of mine to work both with nurses and with doulas to improve the continuity of care, to optimize and support each other’s roles, and to emphasize that we must work together (rather than against one another) to make birth better.
I’ve got a long to-do list, and I’m looking for volunteers.
Thank you to all of you who share my passion, and let’s #keepgoing.
Love, Kate
